
Efficacy and Safety of Pulsed Magnetic Therapy in Sleep related Disorders: A Remote, Randomized, Double-Blind, Placebo-Controlled Trial
Abstract
Background/Aim
Sleep disturbances are common and are associated with impaired daytime functioning, reduced quality of life, and increased health risks. Non-pharmacological neuromodulatory interventions have gained interest as alternatives to hypnotic medication. Pulsed electromagnetic field (PEMF) therapy has been proposed as a non-invasive approach to improve sleep quality and recovery, but evidence from large, well-controlled trials remains limited.
The objective of this study was to evaluate the efficacy and safety of pulsed magnetic field therapy (PMT) on sleep quality, sleep-related symptoms, daytime functioning, and well-being in adults with heterogeneous sleep complaints.
Materials and Methods
In this remote, randomized, double-blind, placebo-controlled trial, 217 adults reporting non-restorative sleep, difficulties initiating sleep, or frequent nocturnal awakenings were assigned to active PMT using a PEMF device (Night Harmony Female/Male protocol) or a sham application for three weeks. Primary outcomes were changes in the Pittsburgh Sleep Quality Index (PSQI) global score and self-rated sleep satisfaction, restfulness, and sleep initiation difficulties. Secondary outcomes included sleep diary measures, daytime functioning, well-being (WHO-5), symptom burden (MYMOP), and daytime sleepiness (Epworth Sleepiness Scale). Analyses followed the intention-to-treat principle using ANCOVA with baseline values of the respective parameter as covariate.
Results
Both groups showed significant improvements over time in global sleep quality and most secondary outcomes (p < 0.001). Between-group differences in PSQI global score were not significant (p = 0.314). However, active PMT resulted in significantly greater improvements in subjective sleep satisfaction (p = 0.02) and restfulness (p = 0.02), particularly among participants with moderate to severe baseline sleep disturbances (p < 0.001 for both). Sleep continuity measures improved similarly in both groups. No serious adverse events were reported.
Conclusions
PMT produced modest but significant improvements in subjective restorative aspects of sleep beyond placebo effects and was well tolerated. Further studies using objective sleep measures and longer follow-up are warranted.
Article Information
- Received
- Accepted
- Published
Academic Editor: Anubha Bajaj, Consultant Histopathologist, A.B. Diagnostics, Delhi, India
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2026 Peter Marmann, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Peter Marmann, Healy GmbH, Kränzlin, Germany —
Competing Interests
The author has the following conflict of interests: The Author Dr. Peter Marmann is an employee of Healy GmbH, the sponsor of the study.
Funding
No specific funding statement was provided by the authors.
Data Availability
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Citation:
Introduction
Sleep quality plays a crucial role in overall health and wellbeing. Sleep disorders encompass a heterogeneous group of conditions characterized by difficulties in initiating or maintaining sleep and by unrefreshing or poor-quality sleep. They are among the most prevalent health complaints globally. Estimates for any sleep problem range from 12% to over 50%, depending on the country, assessment method, and population studied 1, 2, 3, 4. Persistent sleep problems impair cognitive function, mood, and immune regulation and increase the risk of cardiovascular and metabolic diseases5, 6, 7.
Disturbed sleep and related concerns, including trouble initiating sleep, trouble falling asleep and nonrestorative sleep, are common in both general and older populations 8, 9, 10.
Non-pharmacological approaches, including cognitive-behavioral and neuromodulatory interventions, have gained increasing attention as alternatives to hypnotic medications 11, 12. Among these, pulsed electro-magnetic field (PEMF) therapy has been proposed as a non-invasive method to improve sleep quality and general wellbeing by influencing physiological processes related to sleep 13, 14.
Large, double-blind, placebo-controlled trials show that pulsed electromagnetic field (PEMF) therapy can significantly improve sleep quality, particularly at specific frequencies (notably 16 Hz and 1 Hz) 13, 14. Improvements were observed in both subjective sleep quality scores and objective sleep parameters, with effects persisting at least one-week post-treatment 14.
PEMF therapy has also been associated with reduced anxiety and improved overall quality of life, which may further support better sleep 13, 15. Case reports and small studies suggest deeper, more restful sleep and increased alertness as incidental findings after PEMF treatment 15.
In patients with post-COVID-19 fatigue syndrome, PEMF therapy improved insomnia severity and mental health, though the study was small and further research is needed 16.
In people with multiple sclerosis, PEMF did not show significant improvements in fatigue or sleep compared to placebo, indicating that effects may depend on the underlying condition and protocol 17.
PEMF is thought to modulate the autonomic nervous system and brain activity, possibly increasing melatonin secretion and calming neural circuits 11, 12, 16. Studies report PEMF as a non-invasive, well-tolerated therapy with no serious side effects in the short term 13, 14, 18.
PEMF therapy appears to be a promising, non-pharmacological option for improving sleep quality, especially in insomnia and general sleep disturbances. However, more large-scale, high-quality studies are needed to confirm efficacy across different populations and to optimize treatment protocols.
The present study evaluates the efficacy and safety of PMT in adults with distinct types of sleep problems using a remote, stratified, randomized, double-blind, placebo-controlled design. This trial aimed to investigate the effects of PEMF therapy applying McMakin “Night Harmony Female/Male” programs with a PEMF device (MagHealy) on sleep-related parameters, perceived wellbeing, and recovery in healthy adults compared with a sham application. The stratification allows targeted assessment of PMT effects across different symptom clusters, reflecting the clinical heterogeneity of insomnia.
Method and Materials
Study Design
This was a 3-week, remote, randomized, double-blind, placebo-controlled trial conducted entirely through secure digital platforms. All procedures complied with the Declaration of Helsinki. Participants provided electronic informed consent.
The study was designed as a two-armed, double blinded sham-controlled study with a three-week treatment period with a measurement point at the beginning and at the end of the study. A study protocol was finalized before commencement of recruitment. Volunteers were recruited via an existing network of people interested in this type of treatment. After signing the online informed consent form, participants were randomly assigned to one of the two study groups:
Application group (A)
Participants who already use the investigational pulsed magnetic field device in daily routine (existing clients) but are not already having any experience in using the new application designed for improving sleep problems used this new application two times per day for 3 weeks with a frequency range between 5 Hertz and 970 Hertz
Control group (B)
Same as application group A but deactivated PEMF device (sham application)
Participants
Participants were volunteers who have one or more of the sleep related problems non-restorative sleep, problems of falling asleep or frequently awakening at night and would profit from some self-help treatment in their general wellbeing, coping with particular issues, such as sleep problems, low affect or lack of energy. They gave informed consent to participate prior to any study specific procedure.
Volunteers were advised to participate only if they would not violate any restrictions for use as given in the Instructions for Use of the MagHealy device (not intended for pregnant women, persons with epilepsy, heart disease or those with a pacemaker).
Treatment device
According to the MagHealy product specification the device generates a pulsating magnetic field. Key specifications include a frequency range of 0-12.5 MHz, a portable, compact design, and a Bluetooth range of up to 10 meters for app connectivity. It creates an electromagnetic field up to 300 µT.
Treatment application
Participants assigned to group A applied the frequency program Night Harmony Female/Male. This program is especially designed for improving sleep quality. The program was applied according to a predefined treatment plan once per day before going to bed for a total of 3 weeks.
Participants of group B are assigned to use the same program, but the devices of these participants used a placebo program (deactivated device), which enables the LED of the MagHealy device to work normally.
Outcome measures
A combination of validated patient-reported outcome measures and daily electronic sleep diaries were used to assess treatment effects on sleep quality, sleep continuity, mood, daytime functioning, and overall well-being.
Pittsburgh Sleep Quality Index (PSQI)
Sleep quality and functional impact were assessed using the Pittsburgh Sleep Quality Index 19, 20, a validated 19-item instrument evaluating perceived sleep parameters over the previous month. The PSQI yields:
· Global Score (0–21): higher scores indicate poorer sleep quality
· Seven Component Scores, including Sleep latency; Sleep duration, Sleep efficiency, Sleep disturbances, Daytime dysfunction/restorativeness, Sleep quality, Use of sleep medication
PSQI Components 2, 5b, and 7 were prespecified as primary efficacy measures depending on the participant’s enrolled stratum.
Patient Sleep Diary (Adapted From PSQI)
Participants completed a structured daily electronic sleep diary based on PSQI domains, including the following: Sleep onset latency (minutes), Number and duration of nighttime awakenings, Total sleep time (minutes), Time in bed and calculated sleep efficiency (%), Morning restorativeness (0–10 rating scale), Daytime fatigue, alertness, and adverse symptoms (0–10 scales)
Daily sleep diary entries were aggregated into weekly means for efficacy analyses to reduce within-subject variability and improve the stability of outcome measures. This approach minimizes the influence of day-to-day fluctuations in sleep patterns, enhances precision in estimating treatment effects, and aligns the temporal resolution of sleep outcomes with other weekly clinical assessments. Aggregation also mitigates the impact of occasional missing diary entries, providing more robust and interpretable efficacy results.
World Health Organization–Five Well-Being Index (WHO-5)
Measure Yourself Medical Outcome Profile (MYMOP)
Individualized symptom burden and personalized treatment benefit were evaluated using MYMOP 24, 25, 26, enabling each participant to identify their most distressing symptoms and associated functional limitations. Scores for the primary symptom were assessed weekly on a 11-point scale (0 to 10), where higher scores indicate greater severity or impairment.
Epworth Sleepiness Scale (ESS)
Primary Endpoints
The primary efficacy endpoint was the change from baseline to week 3 in the Pittsburgh Sleep Quality Index (PSQI) global score, assessing overall subjective sleep quality.
In addition, the self-assessments of general satisfaction with sleep quality, restfulness of sleep and difficulties falling asleep were evaluated as co-primary endpoints, enabling a multidimensional assessment of treatment effects on specific sleep domains.
Both the global PSQI scores and the self-assessment scores were analyzed as continuous variables using analysis of covariance (ANCOVA) with baseline values as covariates and treatment group as fixed factor. Adjusted mean changes from baseline and between-group differences with 95% confidence intervals were reported.
To preserve interpretability across sleep phenotypes, exploratory subgroup-specific analyses were also conducted to examine differential response patterns among participants with (1) severe difficulty falling asleep, (2) awakening at night, or (3) non-restorative sleep at baseline.
Secondary Endpoints
Secondary efficacy endpoints were evaluated across the entire study population and, where relevant, within each symptom-based stratum. These endpoints were designed to further characterize the impact of pulsed magnetic therapy on sleep continuity, sleep quality, next-day functioning, and psychological symptoms:
Sleep Onset and Maintenance Metrics (Diary-Based)
Awakening at night / frequency
Awakening at night / duration (minutes)
Time until falling asleep (minutes)
Daytime Functioning and Symptom Burden
Restfulness of sleep (1-6; diary)
Daytime exhaustion (1-6; diary)
Daytime stamina (1-6, diary)
Mood and Anxiety Outcomes
Change in WHO-5 (The World Health Organization-Five Well-Being Index) and adapted Mymop (Measure Yourself Medical Outcome Profile), change in Epworth Sleepiness Scale (ESS) total score (Survey)
Safety Endpoints
Safety and tolerability outcomes included: Change in Epworth Sleepiness Scale (ESS) total score (Survey) incidence, severity, and relatedness of Treatment-Emergent Adverse Events (TEAEs) Frequency of treatment discontinuations due to adverse events.
Subgroup Analyses
Subgroup analyses were prespecified in the statistical analysis plan to further characterize treatment effects across clinically relevant patient subsets and to explore potential moderators of therapeutic response. In addition to analyses performed in the overall study population, predefined subgroup analyses were conducted to examine possible differences in efficacy among participants presenting with distinct patterns of sleep disturbance at baseline. The subgroups were defined according to established clinical thresholds derived from the Pittsburgh Sleep Quality Index (PSQI) and a self-reported measure of perceived sleep restoration, perceived sleep quality and difficulties falling asleep.
1. Severe sleep problems: Participants with pronounced sleep problems were defined as those with a PSQI total score at baseline of higher 5 30. This criterion corresponds to a sleep quality typically considered clinically meaningful and indicative of significant insomnia symptoms.
2. Satisfaction with sleep quality, non-restorative sleep and difficulties falling asleep: Participants reporting low subjective satisfaction with sleep, low restoration by sleep and or distinct problems falling asleep were identified as those with a self-assessment score of less or equal to 5 on a 0–10 Likert scale, where higher values denote greater perceived satisfaction by sleep 31. This threshold was selected to capture individuals experiencing notably problems with the corresponding item.
These subgroups were established a priori to assess whether the efficacy of pulsed magnetic therapy varied according to baseline sleep characteristics. The analyses were intended to identify potential modifiers of treatment response and to generate hypotheses for future targeted investigations.
Statistical Analysis
Analyses will follow the intention-to-treat principle.
All primary and secondary efficacy analyses were performed on the intent-to-treat (ITT) population, defined as all randomized participants who completed at least one post-baseline assessment. Statistical significance tests were two-sided with α = 0.05, without adjustment for multiplicity unless otherwise specified in the hierarchical testing plan.
Primary Analysis Approach
For continuous endpoints with normally distributed residuals and sufficient data completeness, analysis of covariance (ANCOVA) was used to compare treatment groups at the primary evaluation timepoint (Week X). Each model included:
· Treatment group (pulsed magnetic therapy vs placebo)
· Baseline value of the endpoint as a covariate
Adjusted mean differences between groups were estimated with 95% confidence intervals.
Longitudinal and Sensitivity Analyses
When repeated measures across time provided greater power or insight, repeated-measures ANOVA or mixed-effects models (MMRM) were used, including:
· Fixed effects for treatment, visit (time), treatment × visit interaction, and baseline
· An unstructured or autoregressive covariance structure, selected by model fit criteria
These models assume data missing at random (MAR).
Non-Parametric Methods
For ordinal variables, non-normal distributions, or endpoints violating parametric assumptions, non-parametric tests were applied, including:
Wilcoxon rank-sum test for between-group comparisons
Wilcoxon signed-rank test for within-group change
Hodges–Lehmann estimator and 95% CI for effect size
Safety Analyses
Safety outcomes were summarized descriptively in the safety population (all participants who initiated treatment). Adverse events were coded and analyzed by incidence, severity, and relatedness.
Missing Data Handling
Surveys
For survey-based instruments (PSQI, WHO-5, MYMOP, Epworth Sleepiness Scale), missing post-baseline data were replaced using last observation carried forward (LOCF). The last available non-missing score was carried forward to all subsequent missing timepoints, provided the participant had at least one post-baseline assessment.
Daily Sleep Diaries
Diary-based data were processed using the following approach:
· Short-term missing days: If ≤3 consecutive diary days were missing within a given week, the missing values were replaced using LOCF from the most recent prior day.
· Extended missing days: If >3 consecutive diary days were missing within a week, the entire weekly summary was treated as missing.
Analyses were performed using validated statistical software (R v4.3.4).
Safety analyses will summarize adverse event frequencies descriptively.
Results
Demographics and Baseline Characteristics
This pilot study was conducted without prior case number estimation. It was assumed that 120 evaluable cases per study group would be sufficient to detect significant group differences.
242 people consented to the study protocol and were randomly allocated to one of both study groups: active study group (A) or to the sham control group (B), resulting in 121 participants in each study group. Because of withdrawal of consent prior to study start, in total 24 participants who have given informed consent but did not participate in the study. 217 participants completed the first survey consisting of the study population according to the ITT principle. 16 participants terminated the study prematurely (8 in each group). Two hundred and one participants completed both surveys and terminated the study according to the protocol.
Since slightly more participants from the control group withdrew consent prior to study start, the groups were somewhat unevenly distributed. The active group consisted of 111 participants, while 106 study participants were assigned to the control group.
16 participants (8 in each group) did not terminate the study regularly and did not complete the final survey. This missing data was replaced according to the last observation carried forward principle.
As can be seen from Table 1, the randomization process yielded quite comparable groups. The majority of the participants, 89%, were female. Due to data-protection concerns age was only collected in rough categories. 70 percent or 80 participants belonged to the middle-aged group between 41 and 60, and nearly half of the rest were older than 60 years or younger than 40 years.
The baseline values of all endpoint parameters differed only marginally in both groups. The respective 95% confidence intervals overlapped and the t-tests for independent samples did not reveal any significant group differences (survey: t = 0.31, p = 0.76 for PSQI, t = 1.96, p = 0.06 for WHO-5; t = 1.52, p = 0.13 for Mymop, t = 1.85, p = 0.07 for ESS; df 215 for each; Diary : t = 1.43, p = 0.15 for restfulness of sleep, t = 1.33, p = 0.18 for awakening frequency; t = 0.59, p = 0.55 for time to fall asleep, t = 0.65, p = 0.52 for daytime tiredness; df 200 for each).
Participant’s compliance was determined by the frequency of study programs used during the study period. This is tracked in a cloud and can be read from there. In both groups, compliance, defined as at least 50% of the intended applications performed, was close to 70%. The two groups differed only very slightly (CHIQU-test, p = 0.89).
Table 1. Baseline characteristics: Gender, age groups, group active application, sham); absolute frequencies and percentages (per category and group); mean scores for PSQI, WHO 5, MYMOP scale and Epworth Sleepiness Scale (95% Confidence Intervals); compliance per treatment group, defined as follows: for both treatment groups at least 50% of the stipulated applications are defined as compliant, less than 5 application were defined as non-compliant.| Active application(n = 111) | Sham application(n = 106) | Total (217) | |
| Gender | |||
| Female | 99 (89%) | 94 (89%) | 193 (89%) |
| Male | 12 (11%) | 12 (11%) | 24 (11%) |
| DNS | 0 (0%) | 0 (0%) | 0 (0%) |
| Age groups | |||
| 20-40 | 12 (11%) | 14 (11%) | 26 (12%) |
| 41-60 | 78 (70%) | 72 (68%) | 150 (69%) |
| Older than 60 | 21 (19%) | 20 (19%) | 41 (19%) |
| Outcome Parameters Baseline (Survey) | |||
| PSQI-Sum Score (0-21) | 9.68(9.0 -10.37) | 9.42 (8.70 – 10.12) | 9.56 (9.07 – 10.05) |
| Satisfaction with sleep (0 – 10) | 5.05 (4.67 – 5.42) | 5.23 (4.92 – 5.55) | 5.14 (4.89 – 5.38) |
| Restfulness of sleep (0 - 10) | 4.55 (4.17 – 4.74) | 4.85(4.47 – 5.05) | 4.70 (4.43 – 4.83) |
| Difficulties falling asleep (0- 10) | 6.05 (5.61 – 6.28) | 5.66 (5.15 – 5.92) | 5.86 (5.53 – 6.03) |
| WHO-5 Score (0-25) | 10.64 (9.93 – 11.35) | 11.78 (10.87 – 12.67) | 11.18 (10.61 – 11.77) |
| MyMop (0-10) | 7.14 (6.53-7.74) - | 6.76(5.93 – 7.58) | 6.97 (6.48 – 7.45) |
| Epworth Sleepiness Scale (0 – 24) | 9.02(8.20 – 43.45) | 7.90(7.01 – 8.78) | 8.48(7.88 – 9.08) |
| Outcome Parameters Baseline (Diary) | |||
| (n = 99) | (n = 103) | (n = 202) | |
| Restfulness of sleep (1-6) | 2.94 (2.78 – 3.12) | 2.77 (2.61 – 2.95) | 2.86 (2.74 – 2.98) |
| Awakening at night / frequency | 2.08 (1.76 – 2.40) | 1.78 (1.46 – 2.10) | 1.93 (1.70 – 2.15) |
| Awakening at night / duration (minutes) | 26.78 (20.48 – 33.08) | 21.78 (17.01 – 26.56) | 24.23 (20.23 – 28.15) |
| Time until falling asleep(minutes) | 25.64 (20.48 – 30.08) | 30.91 (24.77 – 37.05) | 28.32 (24.43 – 32.22) |
| Daytime tiredness (1-6) | 2.38(2.22 – 2.55) | 2.30(2.13 – 2.48) | 2.34(2.22 – 2.46) |
| Compliance | |||
| CompliantNon Compliant | 76 (68 %)35 (32 %) | 79 (75 %) 27 (25%) | 155 (71 %)62 (29%) |
Primary Endpoints
Both active and control groups demonstrated meaningful improvements in overall sleep quality over the study period (Figure 1). Mean reductions in PSQI global score were –3.24 (active) and –2.89 (control), corresponding to a small, non-significant between-group effect (Cohen’s d = 0.14, p = 0.314; Table 2).
Improvements were more pronounced for subjective sleep experiences. Participants receiving active treatment reported significantly greater satisfaction with sleep (mean increase = 1.78 vs. 1.18; Cohen’s d = 0.30, p = 0.029) and restfulness of sleep (mean increase = 2.15 vs. 1.63; Cohen’s d = 0.33, p = 0.042).
Changes in difficulty falling asleep were modest and did not differ significantly between groups (mean decrease = 1.99 vs. 1.78; Cohen’s d = 0.07, p = 0.64).
Collectively, these findings suggest that while pulsed magnetic therapy did not significantly outperform placebo in reducing global PSQI scores, it produced small but statistically significant gains in perceived satisfaction and restfulness of sleep.
Figure 1. Group differences in marginal means of primary endpoint parameters; error bars = 95% CI for Mean Difference.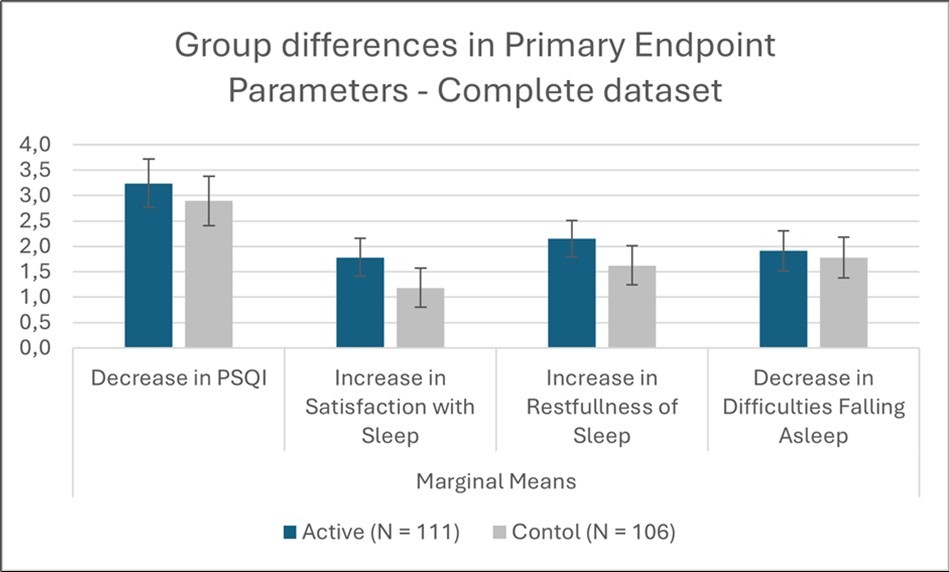
Download figure
| Cases | Sum of Squares | df | Mean Square | F | p |
| PSQI | |||||
| Group | 6.602 | 1 | 6.602 | 1.020 | 0.314 |
| Baseline | 824.876 | 1 | 824.87 | 127.44 | < .001 |
| Residuals | 1.385.05 | 214 | 6.472 | ||
| Satisfaction with sleep | |||||
| Group | 19.296 | 1 | 19.296 | 4.826 | 0.029 |
| Baseline | 276.813 | 1 | 276.81 | 69.230 | < .001 |
| Residuals | 855674 | 214 | 3998 | ||
| Restfulness of sleep | |||||
| Group | 14.910 | 1 | 14.910 | 4.189 | 0.042 |
| Baseline | 207.994 | 1 | 207.99 | 58.441 | < .001 |
| Residuals | 761.640 | 214 | 3.559 | ||
| Difficulties falling asleep | |||||
| Group | 0.961 | 1 | 0.961 | 0.220 | 0.640 |
| Baseline | 286.822 | 1 | 286.82 | 65.596 | < .001 |
| Residuals | 935725 | 214 | 4373 | ||
Subgroup Analysis of Participants with Pronounced Baseline Complaints
A prespecified subgroup analysis was performed among participants who reported pronounced complaints on the corresponding PSQI item at baseline. ANCOVA models adjusting for baseline severity showed that participants in this subgroup experienced larger absolute improvements across all outcomes compared with the full sample.
Reductions in PSQI global score were comparable between groups (marginal mean change: active 3.865; control 3.586), and the between-group difference was not statistically significant (p = 0.501). The estimated effect size was small (Cohen’s d = 0.07).
In contrast, significantly greater improvements were observed for subjective sleeper-centered outcomes. Participants receiving active treatment reported a larger increase in satisfaction with sleep (2.427 vs. 1.770; p = 0.022; Cohen’s d = 0.349) and a markedly larger increase in restfulness of sleep (3.012 vs. 2.078; p = 0.007; Cohen’s d = 0.472). These effect sizes fall within the small-to-moderate range and exceed those observed in the overall sample, indicating that participants with more severe baseline impairment may derive greater benefit.
For difficulty falling asleep, both groups demonstrated substantial improvements (3.323 vs. 3.013), with no significant between-group difference (p = 0.249) and a small effect size (Cohen’s d = 0.20) (Table 3).
Overall, in participants with pronounced baseline symptoms, pulsed magnetic therapy yielded significantly greater improvements in satisfaction and restfulness of sleep, while improvements in global PSQI score and sleep initiation difficulty remained similar to placebo.
Figure 2. Group differences in marginal means of primary endpoint parameters; Subgroups with pronounced problems at baseline; error bars = 95% CI for Mean Difference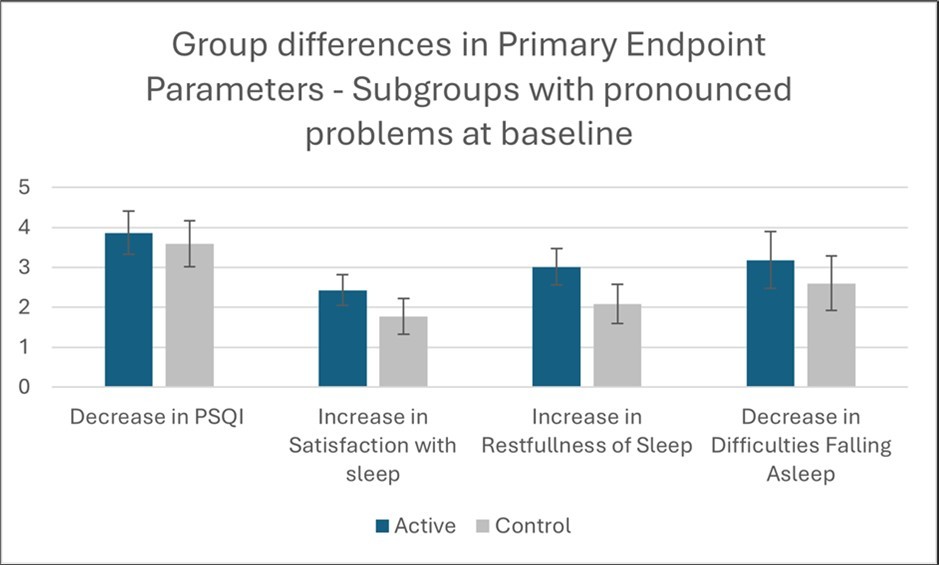
Download figure
| Cases | Sum of Squares | df | Mean Square | F | p |
| PSQI | |||||
| Group | 3.492 | 1 | 3.492 | 0.487 | 0.486 |
| Baseline | 373.239 | 1 | 373.239 | 52.100 | < .001 |
| Residuals | 1.268.019 | 177 | 7.164 | ||
| Satisfaction with sleep | |||||
| Group | 18.674 | 1 | 18.674 | 5.370 | 0.022 |
| Baseline | 73.352 | 1 | 73.352 | 21.094 | < .001 |
| Residuals | 594.634 | 171 | 3.477 | ||
| Restfulness of sleep | |||||
| Group | 30.676 | 1 | 30.676 | 7.585 | 0.007 |
| Baseline | 21.576 | 1 | 21.576 | 5.335 | 0.022 |
| Residuals | 562.126 | 139 | 4.044 | ||
| Difficulties falling asleep | |||||
| Group | 8.733 | 1 | 8.733 | 1.344 | 0.249 |
| Baseline | 7.625 | 1 | 7.625 | 1.174 | 0.281 |
| Residuals | 669.142 | 103 | 6.497 | ||
Secondary endpoints: Sleep Onset and Maintenance Metrics (Diary-Based)
Both treatment groups demonstrated significant improvements over time across all diary-based sleep parameters (Figure 3). The frequency of nocturnal awakenings decreased by an average of 0.65 events per night in the active group during the final study week and by 0.38 events per night in the control group. Despite the numerically greater reduction in the active arm, an ANCOVA adjusting for baseline values found no significant between-group difference (F = 0.663, p = 0.43). The significant time effect in both arms indicates that participants generally experienced fewer nighttime awakenings regardless of treatment conditions.
For duration of sleep interruptions, the active group showed a mean reduction of 4 minutes, compared with a 5.5-minute reduction in the control group. Baseline-adjusted ANCOVA revealed no significant group effect (F = 0.427, p = 0.514).
A comparable pattern was observed for sleep onset latency. Participants in the active group demonstrated a mean decrease of 12 minutes, whereas those in the control group improved by 11 minutes. The between-group comparison again did not reach statistical significance after baseline adjustment (F = 2.392, p = 0.124).
Overall, although sleep diary measures improved over the course of the study in both groups, none of the between-group differences were statistically significant, suggesting that the magnitude of change did not differ reliably between the active pulsed magnetic field intervention and control conditions.
Figure 3. Changes of sleep parameters in the course of the study: a.) Mean change in frequency of awakening at night, b.) duration of interruption, c.) change in time till falling asleep; error bars = 95% CI for Mean Difference 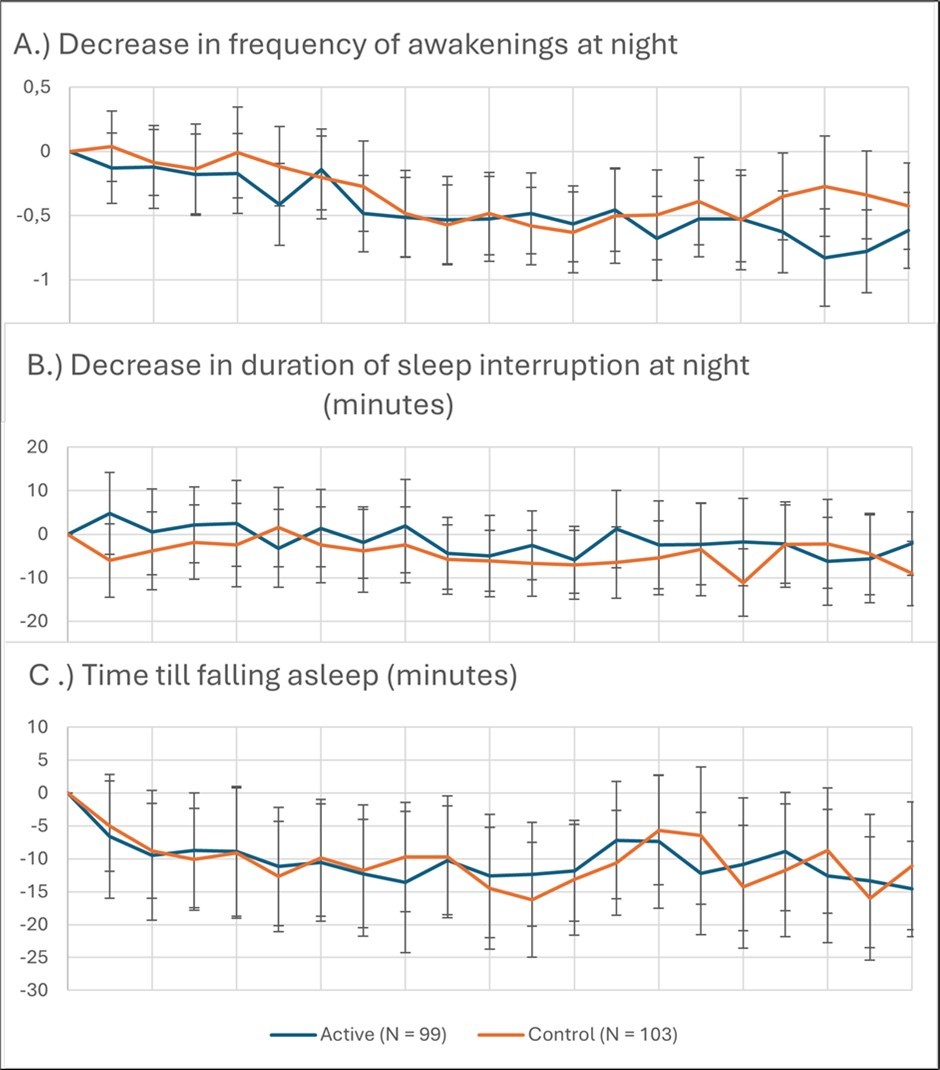
Download figure
Daytime Fitness Outcomes
Diary-based ratings of daytime functioning also improved over the course of the study.
Restoration by sleep increased by 0.65 points in the active group and 0.21 points in the control group (6-point Likert scale). Repeated-measures ANOVA confirmed significant time effects for both the active group (F = 3.18, p < 0.001) and the control group (F = 7.17, p < 0.001). Importantly, baseline-adjusted ANCOVA revealed a significant between-group (Figure 4) difference favoring the active intervention (F = 8.990, p = 0.003).
Daytime stamina improved by 0.66 points in the active group and 0.46 points in the control group. Time effects were significant in both groups (active: F = 18.853, p < 0.001; control: F = 6.559, p = 0.002). However, the between-group difference was not significant in baseline-adjusted ANCOVA (F = 1.330, p = 0.250).
Daytime exhaustion decreased (improved) by 0.54 points in the active group and 0.40 points in the control group. Time effects again reached significance in both groups (active: F = 20.04, p < 0.001; control: F = 5.517, p = 0.005), while ANCOVA showed no significant between-group difference (F = 1.71, p = 0.189).
Figure 4. Changes in sleep related daytime fitness parameters in the course of the study: a.) Mean change in restoration by sleep; b.) Mean change in daytime stamina; c.) Mean change in daytime exhaustion; error bars = 95% CI for Mean Difference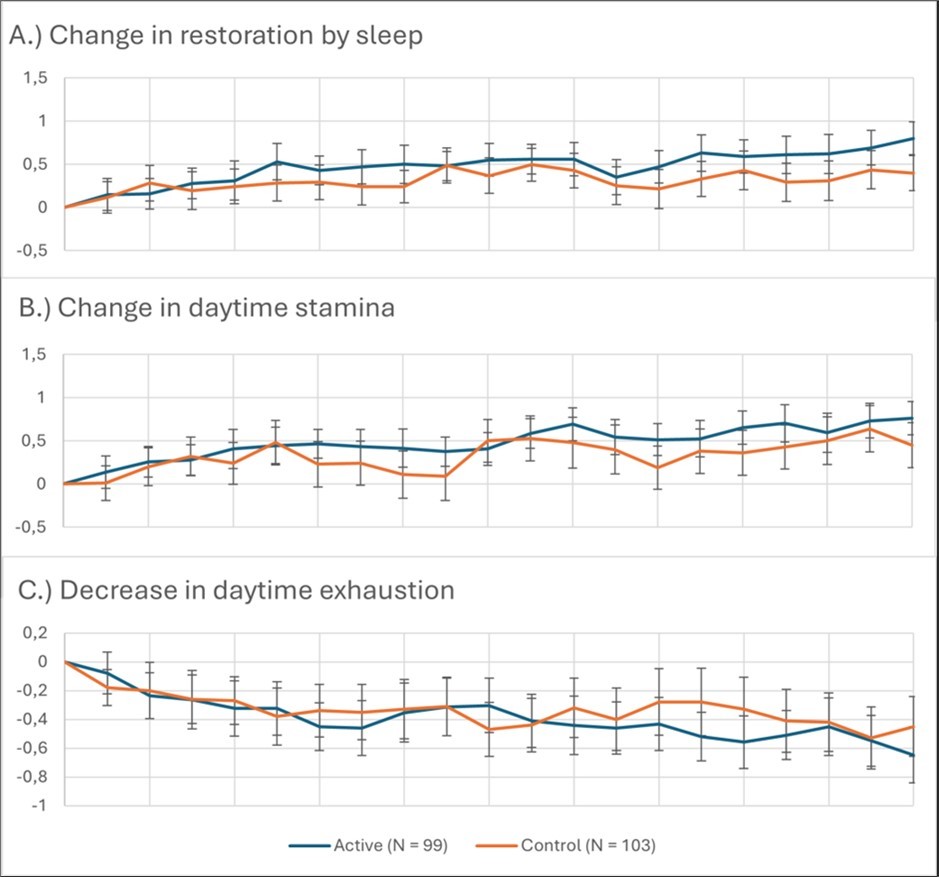
Download figure
Well-Being, Symptom Burden, and Daytime Sleepiness (WHO-5, MYMOP, ESS)
Baseline and post-intervention survey measures demonstrated significant within-group improvements in both the active and control arms.
In the active group, paired-sample t-tests showed robust improvements across all three scales: WHO-5 well-being scores increased significantly (t(110) = 9.192, p < .001), MYMOP symptom scores decreased (t(102) = 7.426, p < .001), and Epworth Sleepiness Scale (ESS) scores also decreased (t(110) = 5.498, p < .001).
The control group likewise showed significant pre–post changes: WHO-5 scores improved (t(105) = 8.074, p < .001), MYMOP scores decreased (t(97) = 4.645, p < .001), and ESS scores decreased (t(105) = 6.015, p < .001).
Despite these substantial within-group improvements, baseline-adjusted between-group comparisons did not reveal significant differences. ANCOVA results indicated no significant treatment effect for WHO-5 (F = 1.091, p = 0.297), MYMOP (F = 1.739, p = 0.189), or ESS scores (F = 0.044, p = 0.835).
Overall, both groups demonstrated meaningful improvements in well-being, symptom burden, and daytime sleepiness across the study interval; however, the magnitude of change did not differ significantly between the active and control conditions (Figure 5).
Figure 5. Group differences in marginal means of secondary endpoint parameters; error bars = 95% CI for Mean Difference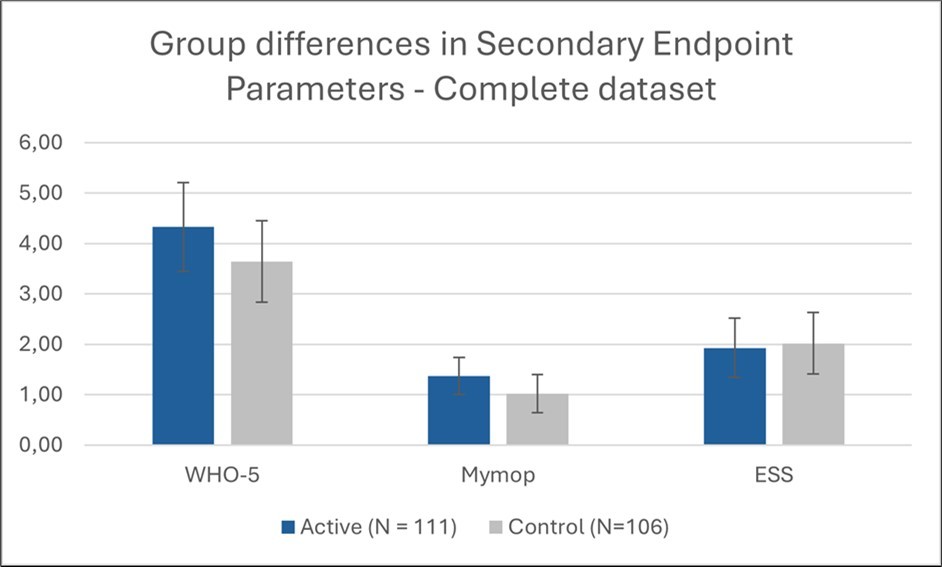
Download figure
Summary of Daytime Results
Taken together, the daytime diary data indicate that participants in both groups experienced improvements in perceived restoration, stamina, and exhaustion across the intervention period. Among these variables, only the sense of restoration by sleep showed a statistically significant between-group difference, favoring the active pulsed magnetic field stimulation.
Safety Results
A total of 46 participants experienced 49 adverse events (AEs) during the study, with 21 AEs in the active group and 28 AEs in the control group. No serious adverse events (SAEs) occurred.
The most frequently reported AEs were upper respiratory infections, including colds (18 cases; 7 active, 11 control) and sinusitis (3 cases; 1 active, 2 control). Musculoskeletal complaints were also common (10 cases total), comprising joint and muscle pain reported in both groups. Allergic reactions occurred in 4 participants (2 per group). Gastrointestinal infections were reported only in the active group (2 cases).
A variety of isolated events were each reported once, including toothache, migraine, elevated blood pressure, stomach pain, endometriosis, influenza, dry skin, unspecified infection, increased urinary urgency, and dizziness. Overall, the distribution and nature of events were consistent with common, self-limiting conditions in the general adult population, with no notable imbalance between study arms.
Adverse Event of Special Interest
One participant in the active treatment group experienced a dermatologic and systemic event considered of special interest due to its temporal proximity to device use. The participant reported the onset of a generalized pruritic rash beginning the day after the first application of the sleep program. Symptoms progressed over several days and were accompanied by nocturnal itching, malaise, cold-sweat sensations, and restlessness. The participant adjusted device intensity parameters but ultimately discontinued use.
The event was also associated with transient lymph node swelling, and symptoms gradually resolved following self-directed management. No clinical diagnosis or confirmatory medical assessment was obtained. The sponsor’s safety officer classified the event as possibly related to treatment, based solely on temporal association, with no evidence of a serious or lasting complication.
Treatment-Related Events
Across the study, three events were judged as having a possible relationship to treatment. Two involved a temporary worsening of sleep problems, one in each treatment arm, both of which improved after discontinuation. The dermatologic event described above represented the third case.
Discussion
This randomized, controlled trial investigated the effects of pulsed magnetic field stimulation on subjective sleep quality, nocturnal sleep continuity, daytime functioning, and well-being in adults with persistent sleep disturbances. Across nearly all outcomes, participants in both the active and control groups showed significant improvements over time. However, only a subset of subjective sleep quality measures demonstrated statistically significant between-group differences favoring the active intervention.
Taken together, the results highlight a dual pattern:
1) robust nonspecific effects across both treatment arms, and
2) small but consistent specific effects of pulsed magnetic field stimulation on selected subjective dimensions—particularly sleep satisfaction, restfulness, and morning restoration.
These selective benefits may reflect subtle neuromodulatory influences on the affective or restorative aspects of sleep rather than on the structural components of sleep continuity. However, they may also reflect expectancy-driven enhancement of subjective sleep perception, especially given the technological nature of the intervention.
Neuromodulators such as acetylcholine, norepinephrine, dopamine, serotonin, histamine, orexin, and melanin-concentrating hormone (MCH) orchestrate sleep-wake states by modulating neuronal activity across brain regions. These systems influence sleep architecture, including transitions between NREM and REM sleep, and regulate processes like memory consolidation and emotional regulation during sleep 32, 33, 34. Serotonin, for example, is implicated in the homeostatic regulation of slow-wave sleep, which is critical for restorative functions 35.
Non-invasive neuromodulation techniques including pulsed magnetic field applications, have shown potential to improve sleep quality, reduce depressive and anxiety symptoms, and enhance restorative sleep features such as sleep efficiency, REM duration, and total sleep time in both clinical and non-clinical populations 36, 37, 38. Some studies report improvements in subjective sleep quality and mood, as well as normalization of stress biomarkers (e.g., cortisol)39. However, objective improvements in sleep architecture are less consistently observed, and placebo effects are notable 40, 41.
Future research should incorporate objective sleep measures (e.g., actigraphy, polysomnography) and examine whether these subjective improvements correspond with physiological changes. Including expectancy assessments, longer follow-up intervals, and mechanistic endpoints will be important for disentangling specific neuromodulatory effects from enhanced placebo responses.
In summary, while pulsed magnetic field stimulation did not produce superior improvements in global sleep quality or sleep continuity, it was associated with modest but statistically significant enhancements in subjective restfulness and sleep satisfaction, especially among participants with more pronounced baseline sleep problems. These findings support the possibility of a subtle treatment-specific effect, superimposed on a large general improvement attributable to placebo and other nonspecific influences.
Limitations
This study has several limitations. Most outcomes were self-reported, making results susceptible to expectancy and reporting bias, which likely contributed to the strong improvements observed in both groups. The lack of objective sleep measures (e.g., polysomnography or actigraphy) limits conclusions about physiological sleep changes. The pronounced placebo response may have reduced sensitivity to detect small treatment-specific effects, and expectancy was not formally assessed. The relatively short intervention period precludes conclusions about long-term efficacy and safety. Subgroup analyses were exploratory and not powered for definitive inference. Finally, adverse events were primarily based on participant reports and were rarely clinically verified, which may underestimate rare or delayed effects.
Conclusion
Pulsed magnetic field stimulation was well tolerated, with no serious adverse events and a similar adverse event profile in the active and control groups. The device demonstrated a favorable short-term safety profile.
Both groups showed substantial improvements in sleep and wellbeing measures, indicating strong nonspecific effects. The intervention did not produce superior outcomes in global sleep quality or sleep continuity. However, subjective sleep satisfaction, restfulness, and morning restoration improved significantly more in the active group, particularly among participants with moderate or greater baseline sleep disturbances.
Overall, pulsed magnetic field stimulation was associated with small but significant benefits in subjective restorative sleep outcomes, while effects on global sleep quality and objective sleep parameters were limited.
Authorship statement
Dr. Peter Marmann (PM) organized the study, recruited the participants and collected the data. He also analyzed the data and wrote the first draft of the manuscript.
Marcus Schmieke (MS) developed the design of the study and finalized the manuscript.
Sponsoring
The study was sponsored by Healy GmbH, Kränzlin, Germany.
Role of the sponsor
The sponsor helped with recruitment by activating his network of users. The sponsor suggested some aspects of the design, like the two active modes of action, superiority of the active group against the untreated control group.
Ethical Statement
This study was conducted in accordance with the principles of the Declaration of Helsinki. It involved healthy adult volunteers and the use of a non-invasive, low risk magnetic field stimulation device intended for general well-being enhancement. The study did not involve any medical intervention, diagnosis, or treatment, and the device used is not classified as a medical device under applicable EU MDR regulations.
In accordance with German research ethics guidelines and institutional policy, no formal ethical approval was required for this type of non-medical, minimal-risk investigation. The study protocol was internally reviewed to ensure compliance with ethical standards, including participant safety, data protection (GDPR), and voluntary informed consent. All participants provided written informed consent prior to enrollment.
Sample availability
The author(s) declare that no physical samples were used in this study.
References
- 1.Léger D, Poursain B, Neubauer D, Uchiyama M. (2008) An international survey of sleeping problems in the general population. , Current Medical Research and Opinion 24, 307-317.
- 3.Nie Q, Shen Y, Luo M, Sheng Z, Zhou R et al. (2023) Analysis of sleep for the American population: Result from NHANES database.. Journal of affective disorders. 10-1016.
- 4.A Van Straten, Weinreich K, Fábián B, Reesen J, Grigori S et al. (2025) The Prevalence of Insomnia Disorder in the General Population: A Meta-Analysis.. Journal of sleep research. 70089-10.
- 5.Medic G, Wille M, Hemels M. (2017) Short- and long-term health consequences of sleep disruption. , Nature and Science of Sleep 9, 151-161.
- 6.Furihata R, Uchiyama M, Takahashi S, Suzuki M, Konno C et al. (2012) The association between sleep problems and perceived health status: a Japanese nationwide general population survey. , Sleep medicine 13, 831-7.
- 7.Sejbuk M, Mirończuk-Chodakowska I, Witkowska A. (2022) Sleep Quality: A Narrative Review on Nutrition, Stimulants, and Physical Activity as Important Factors. Nutrients.
- 8.Stone K, Xiao Q. (2018) . Impact of Poor Sleep on Physical and Mental Health in Older Women.. Sleep medicine clinics 13, 457-465.
- 9.Zhang J, Lam S, Li S, Li A, Wing Y. (2012) The longitudinal course and impact of non-restorative sleep: a five-year community-based follow-up study. , Sleep medicine 13, 570-6.
- 10.Rodrigues R, Nicholson K, Guaiana G, Wilk P, Stranges S et al. (2022) . Sleep Problems and Psychological Well-Being: Baseline Findings from the Canadian Longitudinal Study on Aging. Canadian Journal on Aging / La Revue canadienne du vieillissement 42, 230-240.
- 11.Walker J, Muench A, Perlis M L, Vargas I.Cognitive Behavioral Therapy for Insomnia (CBT-I): A Primer. , Klin Spec Psihol 11(2), 123-137.
- 12.Liu W, Li G. (2025) The Latest Advances in Non-Invasive Neurostimulation for Insomnia: A Review. Nat Sci Sleep. 15, 947-957.
- 13.Jerman I, Škafar M, Pihir J, Senica M. (2025) Evaluating PEMF vagus nerve stimulation through neck application: A randomized placebo study with volunteers. , Electromagnetic Biology and Medicine 44, 173-186.
- 14.Lin P, Lin M, Li W, Zhang C, Li X et al. (2023) . Efficacy and Safety of Pulse Magnetic Therapy System in Insomnia Disorder: A Multicenter, Randomized, Double-Blind, Placebo-Controlled Trial. Psychiatry Investigation 20, 559-566.
- 15.Borges B, Esposito S. (2019) Effects of PEMF (pulsed electromagnetic fields) treatment on a 68-year-old female with moderate anxiety, chronic neck and low back pain and small vessel ischemia.Frontiers in Neurology.
- 16.Keilani M, Steiner M, Sternik J, Schmeckenbecher J, Zwick R et al. (2025) Feasibility, acceptance and effects of pulsed magnetic field therapy in patients with post-COVID-19 fatigue syndrome : A randomized controlled pilot study.. Wiener klinische Wochenschrift. 10-1007.
- 17.Granja-Domínguez A, Hochsprung A, Luque-Moreno C, Magni E, Escudero-Uribe S et al. (2022) Effects of pulsed electromagnetic field therapy on fatigue, walking performance, depression, and quality of life in adults with multiple sclerosis: a randomized placebo-controlled trial.. Brazilian journal of physical therapy. 26, 100449-10.
- 18.Lin D, Zeng Z, Liu J, Long H. (2024) Application of low-frequency pulsed magnetic induction technology in the field of deep sleep. 2024 5th International Conference on Artificial Intelligence and Electromechanical Automation (AIEA) 1068-1071.
- 19.Buysse D J, Reynolds CF 3rd, Monk T H, Berman S R, Kupfer D J. (1989) The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 28(2), 193-213.
- 20.Carpi M. (2025) The Pittsburgh Sleep Quality Index: a brief review. Occup Med (Lond). 75(1), 14-15.
- 21.Sischka P E, Martin G, Residori C, Hammami N, Page N et al.. Cross-National Validation of the WHO-5 Well-Being Index Within Adolescent Populations: Findings From 43 Countries. Assessment. 2026 Jan;33(1): 3-26.
- 22.Topp C W, Østergaard S D, Søndergaard S, Bech P. (2015) The WHO-5 Well-Being Index: a systematic review of the literature. Epub , Psychother Psychosom 84(3), 167-76.
- 23. (2014) . World Health Organisation, Mental health – a state of well-being, ed. Geneva: World Health Organization .
- 24.Paterson C. (2004) Seeking the patient's perspective: a qualitative assessment of EuroQol, COOP-WONCA charts and MYMOP. Qual Life Res. 13(5), 871-81.
- 25.Paterson C, Britten N. (2000) In pursuit of patient-centred outcomes: a qualitative evaluation of the 'Measure Yourself Medical Outcome Profile'. J Health Serv Res Policy. 5(1), 27-36.
- 26.Paterson C. (1996) Measuring outcomes in primary care: a patient generated measure. MYMOP, compared with the SF-36 health survey. BMJ 312(7037), 1016-20.
- 27.Ibáñez Vanessa, Silva Josep, Cauli. (2018) A survey on sleep questionnaires and diaries". , Omar, Sleep Medicine 42, 90-96.
- 28.Johns M W. (1991) A new method for measuring daytime sleepiness: the Epworth sleepiness scale". , (PDF). Sleep 14(6), 540-5.
- 29.Fabbri M, Beracci A, Martoni M, Meneo D, Tonetti L et al. (2021) Measuring Subjective Sleep Quality: A Review. , Int J Environ Res Public Health 18(3), 1082-10.
- 30.The EpworthSleepiness Scale: What the Epworth Sleepiness Scale is and how to use it". Archived from the original on. 2012-03.
- 31.Purbasari P.Pittsburgh Sleep Quality Index (PSQI) Form Administration Instructions, References, and Scoring Form Administration Instructions.
- 33.Sulaman B, Zhang Y, Matosevich N, Kjærby C, Foustoukos G et al. (2024) Emerging Functions of Neuromodulation during Sleep. , The Journal of Neuroscience 44, 10-1523.
- 36.Sørensen N, Haahr U, Larsen M, Hansen J, Nyholm S et al. (2025) Active versus sham transcranial pulsed electromagnetic field headband treatment for major depression: protocol for a double-blinded randomised trial. , BMJ Open 15, 10-1136.
- 37.Sun N, He Y, Wang Z, Zou W, Liu X. (2020) The effect of repetitive transcranial magnetic stimulation for insomnia: a systematic review and meta-analysis.Sleep medicine.
- 38.Sun S, Yuan F, Song L, Liu X, Zhong T et al. (2025) Effectiveness and safety of different electromagnetic stimulation therapies in treating post-stroke insomnia: A network meta-analysis of randomized controlled trials. , PLOS One 20, 10-1371.
- 39.Báez-Suárez A, Báez-Suárez V, Saldanha L, Vílchez-Barrera M, Hernández-Pérez A et al. (2025) Improving Sleep Quality and Well-Being in Institutionalized Older Adults:. , The Potential of NESA Non-Invasive Neuromodulation Treatment. Geriatrics 10, 10-3390.