
Apomorphine Subcutaneous Infusion is More Efficient Than foslevodopa/foscarbidopa Subcutaneous Infusion in the Treatment of Advanced Parkison´s Disease for the Spanish National Health System
Abstract
Objectives
Motor fluctuations and non-motor disorders not manageable by first-line treatments in advanced Parkinson's disease require continuous dopaminergic stimulation strategies such as subcutaneous infusions of apomorphine (APO) or foslevodopa/foscarbidopa (FLD/FCD). A Budget Impact Analysis (BIA) was performed to estimate the cost difference between both treatments assuming equivalent clinical efficacy and safety.
Material and methods
The efficacy results of pivotal clinical trials at 12 and 52 weeks of treatment and the safety profile of APO vs FLD/FCD were compared, based on latest scientific publications and other available clinical data. A comparative BIA was performed, based on estimated annual drug treatment costs at Spanish published prices.
Results
The efficacy of APO (16 h/day) and FLD/FCD (24 h/day) in reduction of OFF hours (2.47 vs 2.75, 12 weeks; 3.66 vs 3.50, 52 weeks; respectively) and increase of ON hours without disabling dyskinesias (2.77 vs 2.72, 12 weeks; 3.31 vs 3.80, 52 weeks; respectively) could be considered clinically equivalent, as well as their safety profiles.
However, a significant discrepancy is observed in the costs of the aforementioned alternatives. Considering published prices and the average dose reported in the literature, in Spain the annual cost of APO would be €13,980 compared to €55,198 for FLD/FCD. Consequently, the financial resources required for the treatment of FLD/FCD would enable the treatment of approximately three to four patients with APO. The BIA indicated the potential for annual savings in more than €2,500 million, considering a total target population of over 60,000 patients per year. Finally, an univariant sensitivity analysis was performed, considering a scenario in which the hospital acquisition cost of FLD/FCD decreased between 20%-30% (€44,159- €38,638/year). In this scenario, the total annual savings range between €1,875-€1,532 million per year.
Conclusions
Overall APO is more efficient than FLD/FCD, as it provides similar clinical efficacy at a lower treatment cost. The selection of an appropriate treatment option is to be determined by clinical criteria and patient characteristics, but cost evaluation should be considered to select the most cost-effective therapeutic option.
Article Information
- Received
- Accepted
- Published
Academic Editor: Anubha Bajaj, Consultant Histopathologist, A.B. Diagnostics, Delhi, India
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2026 Gonzalez J, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Gonzalez J, Medical Department, ITF Research, S.L. Alcobendas (Madrid) —
Competing Interests
GJ is an employee of ITF Research Pharma, S.L.U., Madrid, Spain. DJ is an employee of Keylates Health Solutions, S.L. MM has received honoraria for participation and medical advisory of the study; and for the review of the present manuscript.
Funding
This study was funded by ITF Research Pharma, S.L.U.
Data Availability
The original data and materials that have supported the completion of this study are available.
Acknowledgements
The authors would like to acknowledge Keylates Health Solutions, S.L. for their support in the performing of this study.
Citation:
Introduction
Neurodegenerative diseases (ND) are significant causes of mortality and morbidity worldwide, especially in the elderly population. Among these, Parkinson’s disease (PD) is the second most common ND after Alzheimer’s disease (AD)1 and affects around 160,000 people in Spain2. As PD prevalence increases with age, and given the growing life expectancy, the number of people affected by PD is expected to rise substantially in the future3. In fact, within the ND considered in the Global Burden of Disease, Injuries and Risk Factors Study, PD showed the fastest growth in terms of prevalence, disability and deaths4.
The average age of onset is 60 years old and the mean duration of the disease from diagnosis to death is 15 years1. PD is clinically defined by the presence of bradykinesia and other cardinal motor symptoms. However, most PD patients suffer from non-motor symptoms as well, which significantly contribute to overall burden. Cognitive dysfunction, depression and autonomic failure are some of the most common and relevant non-motor related problems5.
Oral dopaminergic replacement, including levodopa (LD) and/or other antiparkinsonian drugs, is considered the gold standard first line for the treatment of PD. However, as the disease progresses, plasma bioavailability of oral antiparkinsonian drugs may be altered, which leads to an unpredictable response to treatment. Consequently, motor and/or non-motor fluctuations may occur whereby patients alternate between achieving adequate symptom control (“ON” time) or inadequate control (“OFF” time). LD-related fluctuations in PD are associated with disease progression and non-physiological, discontinuous, or pulsatile stimulation of striatal dopaminergic receptors; and may result in unwanted motor symptoms known as dyskinesias6. At this time of the evolution of the disease, infusion therapies become an alternative to oral medication for patients with advanced PD when symptoms are inadequately controlled, as recent European Academy of Neurology/Movement Disorder Society guidelines indicate7.
In these cases, management of the disease requires the use of second-line therapies or Device-Aided Therapies (DAT) such as apomorphine (APO) or foslevodopa/foscarbidopa (FLD/FCD) subcutaneous infusions, among others.
PD, as the second most prevalent ND, leads to high health care costs in the Spanish population. The severity of the disease and the degree of disability caused by both motor and non-motor symptoms contribute significantly to an increase in health-related costs. In this context, the evaluation of the use of advanced therapies in PD becomes critical8. Thus, the aim of this analysis was to assess the budget impact considering the drug costs of APO compared to that of FLD/FCD in patients with advanced stage of PD in Spain.
Methods
Study design and model structure
A Budget Impact Analysis (BIA) is a type of economic evaluation to estimate the financial consequences of adopting a new medicinal product versus the current treatment, showing potential costs or savings for the healthcare system. Costs or savings depend not only on direct costs but also on the expected utilization and uptake of the new intervention.
For performing our BIA, a computer model was designed to assess treatment costs among PD patients treated with APO compared to those treated with FLD/FCD. The base scenario included a three-year time horizon where the payer’s perspective was considered (mainly cost for the Spanish National Healthcare System -SNHS- and patients through minimum co-payment).
The number of patients with PD in Spain is estimated to be around 160,0002, based on the data from the Spanish Society of Neurology. To calculate the number of patients with advanced PD, the prevalence rate was taken from the PARADISE Study9, carried out between 2017 and 2019. The study estimated a prevalence rate of 38.2%, based on data from patients treated in the SNHS. Therefore, our model estimated that the target population for these treatments could reach between 61,000 - 62,000 patients in the next 3 years, according to the expected population increase in Spain10(see Table 1). In this model, we are assuming a theoretical scenario in which every advanced PD patient could be treated, among all available DAT, specifically with APO or FLD/FCD.
Table 1. Target population. APO: apomorphine; FLD/FCD: foslevodopa/foscarbidopa; PD: Parkinson’s disease.The model has been designed as a virtual calculator which includes several variables, such as the number of patients and their daily dose in miligrams (mg) or mililiters (ml); the number of infusion units per year; the number of packages per year; the package Public Price (VAT – Value Added Tax- included) for APO, or the package hospital acquisition cost for FLD/FCD at EX-Factory (EXF) price; and finally, the annual cost in euros for each treatment option.
Clinical comparison between APO and FLD/FCD
In order to ensure clinical consistency in the comparative analysis of the cost of the two therapies, a comprehensive comparison of the profiles of the patients included in the pivotal clinical trials was conducted11, 12. These patients were deemed to be clinically equivalent with respect to the most significant parameters, including age, time since diagnosis of PD, number of daily OFF hours, number of daily ON hours without disabling dyskinesias, and daily dose in LD equivalents (see Table 2). Since these patients were treated with APO or FLD/FCD in their respective (and different) clinical trials, a statistical comparison of sample sizes was not appropriate.
Table 2. Comparison of the profile of PD patients included in the clinical trials. PD: Parkinson’s disease.In terms of clinical comparison, although there is lack of direct comparative trials of the clinical outcomes of APO over those of FLD/FCD, both have shown satisfactory efficacy and safety results in their respective published pivotal randomized, double-blind, controlled clinical trials.
The efficacy of APO (16 h/day perfusion) and FLD/FCD (24 h/day perfusion) in reducing hours of OFF time (2.4711 vs 2.7512, 12 weeks; 3.6614 vs 3.5013, 52 weeks; respectively) and increasing hours of ON time without disabling dyskinesias (2.7711 vs 2.7212, 12 weeks; 3.3114 vs 3.8013, 52 weeks; respectively) could be considered clinically equivalent (see Table 3).
Table 3. Comparison of efficacy between APO and FLD/FCD. APO: apomorphine; CD: carbidopa; LFD/FCD: foslevodopa/foscarbidopa; LD: levodopa.| 12 weeks | 52 weeks | |||
| APO (n=53) 11 | FLD/FCD (n=74) 12 | APO (n=84) 14 | FLD/FCD (n=244) 13 | |
| Daily treatment time (hours) | 16 | 24 | 16 | 24 |
| Daily OFF decrease (hours) | 2.47; (placebo: 0.58) | 2.75; (oral LD/CD: 0.96) | 3.66 | 3.50 |
| Daily ON increase without disabling dyskinesias (hours) | 2.77; (placebo: 0.80) | 2.72; (oral LD/CD: 0.97) | 3.31 | 3.80 |
In terms of safety (see Table 4), we observed some differences in favour of APO in terms of incidence of severe/serious adverse effects at 52 weeks, treatment withdrawals due to adverse effects at 12 and 52 weeks, infusion site erythema, and hallucinations; and favourable to FLD/FCD in terms of skin nodules at infusion site.
Table 4. Comparison of safety between APO and FLD/FCD. APO: apomorphine; FLD/FCD: foslevodopa/forcarbidopa.| 12 weeks | 52 weeks | |||
| APO (n=53) 11 | FLD/FCD (n=74) 12 | APO (n=84) 14 | FLD/FCD (n=244) 13 | |
| Patients with at least one adverse effect (%) | 93 | 85 | 98.8 | 94.3 |
| Patients with severe/serious adverse events (%) | 24 | 17 | 25.0 | 51.6 |
| Patients withdrawing due to adverse effects (%) | 11 | 22 | 16.7 | 26.2 |
| Skin nodules at infusion site (%) | 44 | 8 | 54.8 | 28.7 |
| Infusion site erythema (%) | 17 | 27 | 13 | 52 |
| Hallucinations (%) | 2/53= 3.8 | 11/74= 15 | NR | 42/244= 17.2 |
Posology
The requested dose of APO infusion may vary depending on the needs of each patient. According to the APO Summary of Product Characteristics (SPC)15, the dosage of APO is based on the number of mg per hour that should be continuously infused to achieve the optimal clinical response. Therefore, the infusion should provide a specific number of mg per day of APO, depending on the perfusion flow rate, which is expressed in mg per hour, and the number of hours per day of perfusion. In the case of FLD/FCD, however, it is administered as a continuous subcutaneous infusion with no overnight-pause intervals, so a 24-hour period has been considered to estimate the daily dose for patients receiving this alternative. According to the FLD/FCD SPC16, the dosage is derived from the estimation of the equivalent dose of LD in mg, which needs to be converted to the infusion flow rate of FLD/FCD to optimize the clinical response, expressed as ml of solution per hour. Consequently, the perfusion provides a predetermined volume of solution for FLD/FCD infusion over the course of 24 hours.
Results
Base case and scenario analysis
According to the available literature11, the average daily dosage of APO is 4.68 mg per hour, which at a daily perfusion rate of 16 hours, equates to an average daily dosage of 74.88 mg per day. From a payer´s perspective, we have to consider that in Spain APO is a pharmaceutical product that is dispensed through retail pharmacy as for Public Price (VAT included). Since the Public Price (VAT included) of a package of APO with 5 infusion units (100 mg of apomorphine per infusion unit) is €255.7517, the average annual cost (365 days) would be €13,980 €. Additionally, considering that the lowest dosage in APO’s SPC15 is 1 mg/hour, the total annual treatment cost would be €2,987. Conversely, the highest annual treatment cost is calculated according to a maximum dosage of 100 mg/day. In this case, the total annual treatment cost would amount to €18,670.
For FLD/FCD, we have taken the EXF price (VAT included), as the product is dispensed through the hospital. Based on data available in published literature13, the average dose of FLD/FCD is 1,621.90 mg of LD equivalents. According to FLD/FCD SPC16, this dose equates to an infusion flow rate of 0.55 ml/h, resulting in a daily administration of 13.2 ml of infusion solution.
The average annual cost of treatment at an EXF price (VAT included) of €801.96 per pack with 7 infusion units (2,400 mg foslevodopa and 120 mg foscarbidopa per infusion unit)17 results in a total annual cost of €55,198. Moreover, considering that the lowest dosage is 0.15 ml/hour at 24 hour of infusion, the total annual treatment cost would be €15,054. Conversely, the highest annual treatment cost is calculated according to a maximum dosage of 1.04 ml/h. In this case, the total annual treatment cost would amount to €104,374 €.
Budget Impact Analysis (BIA)
In our BIAmodel, we have just considered the drug cost and 100% uptake of the new intervention FLD/FCD versus APO. In this sense, our BIA shows that switching the treatment of advanced PD patients from FLD/FCD to APO would generate total savings of more than €2,500 million per year, as the cost of treatment with FLD/FCD is nearly 4 times more expensive than APO (€55,198 vs €13,980). Applying this impact at an individual level, switching treatments from FLD/FCD to APO would mean an additional annual saving of €41.218 per patient. See Table 5 for full results.
Table 5. Budget Impact: APO vs FLD/FCD. APO: apomorphine; FLD/FCD: foslevodopa/forcarbidopa.| Year 1 | Year 2 | Year 3 | ||||
| APO | FLD/FCD | APO | FLD/FCD | APO | FLD/FCD | |
| Number of patients (n) | 61,136 | 61,636 | 62,132 | |||
| Cost of treatment (euros) | €13,980 | €55,198 | €13,980 | €55,198 | €13,980 | €55,198 |
| Total cost (million euros) | €855 | €3,375 | €862 | €3,402 | €869 | €3,430 |
| Savings (million euros) | €2,520 | €2,540 | €2,561 | |||
Sensitivity analysis
Univariant sensitivity analysis has been performed to determine the robustness of the results of this model. Minimum, maximum, and average annual costs have been considered for both treatments. Furthermore, a hypothetical scenario has been explored in which the Net Selling Price (NSP) of the hospital drug (FLD/FCD) is set at 20 – 30% below the current official list price. In the base case, the annual treatment cost will range from €15,054 – 104,374 (average €55,198). In the event of a 20% reduction in the EXF price, the annual cost of treatment for FLD/FCD would range from €12,043 to €83,501 (average cost €44,159), whereas a further 30% reduction in the EXF price would result in annual treatment costs for FLD/FCD ranging from €10,538 to €73,062 (average cost €38,638). As illustrated in Figure 1, the financial burden of treatment varies according to the specific scenario under consideration.
Figure 1. Sensitivity analysis and annual costs for APO and FLD/FCD. APO: apomorphine; FLD/FCD: foslevodopa/forcarbidopa.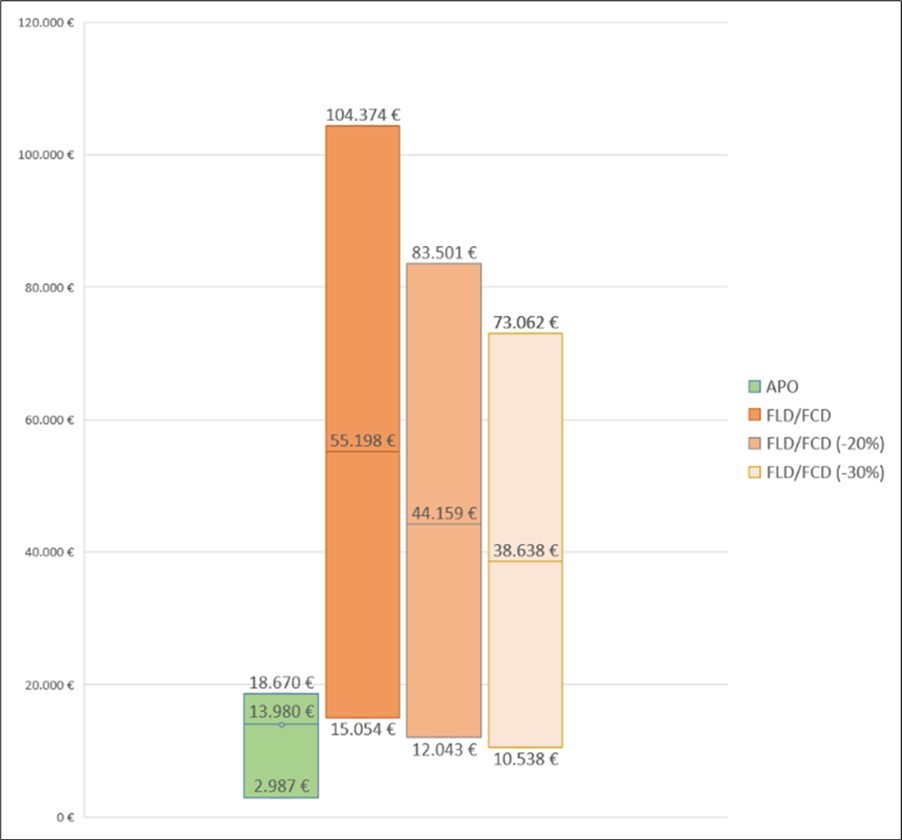
Download figure
Discussion
According to our model, treating patients with advanced PD with APO is a cost-efficient strategy, as SNHS could save and average amount of €42,218 per patient/year considering the administration of APO instead of FLD/FCD and potential annual savings of more than €2,500 million. In the scenario that price reductions of 20% / 30% were applied over current EXF price of FLD/FCD, savings will be of €30,179 / €24,658 per patient/year, respectively. In these scenarios, the total annual savings will range between €1,875-€1,532 million per year.
It is noteworthy that a post-hoc analysis of data from APO pivotal clinical trials was conducted along with an analysis of real-world experience from 13 movement disorders specialists using a questionnaire that focused on starting patients on APO infusion. The specifications of the clinical trial protocols limited individual decision making, as centres were not allowed to proceed with dose adjustments after the first four weeks of double-blind treatment. Nevertheless, real-world data reported that a stable dose of APO was achieved in most patients within 3 weeks18.
APO remains the only drug with efficacy comparable to that of LD. In a crossover open-label study, no difference was observed between APO and LD in all outcome variables, including hand tapping scores, walking time, severity of tremor, dyskinesia score, and a PD disability scale. This study demonstrated for the first time that APO shows the same efficacy on motor symptoms compared with LD, but with a significantly faster onset effect19.
Although data are available to support the efficacy and safety of both APO and FLD/FCD, not all scientific societies or regulatory organizations position them equally. In fact, according to the National Institute of Health Care and Excellence (NICE) of United Kingdom (UK) latest guidelines, and in line with the conclusions of our study, FLD/FCD is recommended only when available medicines for advanced PD are not working well enough, patients cannot be treated with APO or deep brain stimulation (DBS), or if these treatments no longer control symptoms20. Similar conclusions have been reached by the Haute Autorité de Santé (HAS) in France21.
In Spain, despite the efficacy of APO and FLD/FCD, which could be considered clinically equivalent in terms of reduction in hours of OFF time (2.47 vs 2.75, 12 weeks; 3.66 vs 3.50, 52 weeks; respectively) and increase in hours of ON time without disabling dyskinesias (2.77 vs 2.72, 12 weeks; 3.31 vs 3.80, 52 weeks; respectively), treatment-costs show significant differences.
A comparative analysis of the safety data published from the pivotal clinical trials, considered comparable in terms of patients´ profile, primary endpoints, and other clinically relevant parameters, reveals differences that could be significantly favourable to APO in terms of reduced incidences of severe/serious long-term adverse effects, treatment withdrawal due to adverse effects, infusion site erythema, and hallucinations.
Conversely, according to the published data, FLD/FCD had a lower incidence of skin nodules at infusion site. Anyway, it is noteworthy that the skin nodules incidence related to APO treatment has been significantly reduced in recent years in routine clinical practice due to the adoption of minimally invasive Teflon needles22.
Moreover, the apparent lower incidence of hallucinations associated with APO is of outstanding clinical relevance. This finding has been postulated to be due to the pharmacological profile of APO as antagonist of the serotonergic 5-HT2A receptor, pointed in a real-world data comparative study23. This study compared APO with intrajejunal LD/CD infusion (IJLI) and deep brain stimulation of the subthalamic nucleus (STN-DBS). The results showed that APO reduced the perceptual disorders/hallucinations domain of the NMSS (Non-Motor Symptom Scale) to a greater extent than the other two advanced therapies (relative change was -50.9, -34.6 and -55.5 for IJLI, STN-DBS and APO, respectively)23. In this regard, it is also noteworthy that APO is a dopaminergic agonist with very low affinity for the dopaminergic D3 receptor, which has been associated with a lower risk of developing impulse control disorders24, 25.
A comparative study was published in 2020 to analyse the costs of DBS, IJLI, and APO. The methodology used was based on real-world data obtained from an integrated healthcare organization in the Basque Country (Spain) from 2016 to 2018. The study showed the annual cost over 3 years and the projected cost for 2 additional years. The total cost for 5 years’ treatment was €53,217 for DBS, €208,163 for IJLI, and €170,591 for APO, which revealed a considerable higher cost for LD/CD, compared to APO26. Moreover, although DBS seemed to be the most affordable among the three alternatives, a 5-year prospective clinical comparative study between DBS and APO reported a worsening of the Neuropsychiatric Inventory Questionnaire in the DBS group but not in the APO group27.
As a chronic progressive disease in which most patients reach an advanced stage after 7 to 10 years from diagnosis5, PD has a great impact on patients’ and caregivers’ lives. PD caused more than 200,000 deaths and 3,2 million disability-adjusted life-years (DALYs) worldwide in 2016, and more than 4,000 deaths and 54,175 DALYs in Spain4. Moreover, it also involves a substantial social burden and entails an important economic impact. According to data from Parkinson's Survey Observing the Quality of Care (EPOCA) Study conducted in Spain, more than half of the patients are diagnosed of PD between 1-5 years after the first symptom, which means a considerable delay3. These data even further emphasize the importance of having cost-effective therapies for patients in advanced stages, as many of them are diagnosed after having already gone through the early stages of the disease.
According to a survey carried out among neurologists attending PD patients in Catalonia area (Spain), 70% stated that they had some limitation for the implementation of second-line therapies, and the main cause were the lack of resources at their hospital centre (38.1%). Lack of knowledge about second-line therapies or existing circuits for this purpose were also mentioned, among others. Only 7.1% and 2.4% of the neurologists considered the following as limitations to establish second-line therapies: possible side effects or low therapeutic benefit, respectively28.
Finally, it is also noteworthy that a recently published indirect treatment comparison and cost-minimisation analysis conducted from a UK healthcare payer´s perspective has reached similar conclusions to ours in terms of comparative efficacy and safety, as well as cost savings of medication, between APO and FLD/FCD treatments29.
All these previous investigations highlight the importance of access to second-line therapies and the need for affordable treatments for PD patients in Spanish hospitals, in which cost-effectiveness treatments could significantly increase the number of patients benefited from advanced therapies.
This model presents some limitations. The clinical data used to populate the model have been extracted from the literature with different timelines and methodologies and not from real-word studies. Furthermore, the costs used in the model are those available at public databases and may not reflect the real clinical practice or may suffer changes in the future. Moreover, this model does not consider adjuvant medication costs in advanced PD such as levodopa, catechol-O-methyl-transferase inhibitors (iCOMT), monoamine oxidase inhibitors (IMAO), or amantadine, among others; healthcare costs; nor indirect costs; so the indirect savings that APO or FLD/FCD could have achieved in terms of productivity loss may not be reflected in the current results.
Conclusion
Overall, our APO or FLD/FCD medication cost model suggests that APO can be more efficient than FLD/FCD in the treatment of advanced Parkison´s disease from the payer´s perspective of SNHS since treating patients with APO would lead to considerable treatment savings. This goes in line with the recommendations from the guidelines on pharmacological efficiency, recently published by NICE20 or other similar studies29. Although the selection of an appropriate treatment option is mainly to be determined by clinical criteria and patient characteristics, the fact that APO is more affordable than FLD/FCD should be considered for a wise choice of treatment.
Authors’ contributions
All authors contributed to the study. GJ wrote the outline of the manuscript. DJ and MM revised and approved the outline. All authors read and approved the final manuscript.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
References
- 1.Erkkinen M G, Kim M O, Geschwind M D.Clinical Neurology and Epidemiology of the Major Neurodegenerative Diseases. Cold Spring Harb Perspect Biol. 10(4), 033118.
- 2.Neurología Sociedad Española de. (2025) La enfermedad de Parkinson es la enfermedad neurológica que más aumenta en prevalencia, mortalidad y discapacidad en el mundo.
- 3.Santos García D, Blázquez-Estrada M, Calopa M, Escamilla-Sevilla F, Freire E et al.. Present and Future of Parkinson's Disease in Spain: PARKINSON-2030 Delphi Project. Brain Sci 11(8), 1027.
- 4.BD. (2016) Parkinson's Disease Collaborators. Global, regional, and national burden of Parkinson's disease, 1990-2016: a systematic analysis for the Global Burden of Disease Study. , Lancet Neurol 17(11), 939-953.
- 5.Poewe W, Seppi K, Tanner C M, Halliday G M, Brundin P et al. (2017) Parkinson disease. Nat Rev Dis Primers. 3, 17013.
- 6.T Van Laar, Chaudhuri K R, Antonini A, Henriksen T, Trošt M.Infusion Therapies in the Treatment of Parkinson's Disease. , J Parkinsons Dis 13(5), 641-657.
- 7.Deuschl G, Antonini A, Costa J, Śmiłowska K, Berg D et al.European Academy of Neurology/Movement Disorder Society - European Section guideline on the treatment of Parkinson's disease: I. Invasive therapies. , Eur J Neurol 29(9), 2580-2595.
- 8.García-Ramos R, López Valdés E, Ballesteros L, Jesús S, Mir P.Informe de la Fundación del Cerebro sobre el impacto social de la enfermedad de Parkinson en España. , Neurologia 31(6), 401-13.
- 9.Martínez-Castrillo J C, Martínez-Martín P, Burgos Á, Arroyo G, García N et al.. Prevalence of Advanced Parkinson's Disease in Patients Treated in the Hospitals of the Spanish National Healthcare System: The PARADISE Study. Brain Sci 11(12), 1557.
- 10. (2025) Instituto Nacional de Estadística [Internet]. Proyecciones de Población 2022-2072 [last date of access:.
- 11.Katzenschlager R, Poewe W, Rascol O, Trenkwalder C, Deuschl G et al.Apomorphine subcutaneous infusion in patients with Parkinson's disease with persistent motor fluctuations (TOLEDO): a multicentre, double-blind, randomised, placebo-controlled trial. , Lancet Neurol 17(9), 749-759.
- 12.Soileau M J, Aldred J, Budur K, Fisseha N, Fung V S et al.Safety and efficacy of continuous subcutaneous foslevodopa-foscarbidopa in patients with advanced Parkinson's disease: a randomised, double-blind, active-controlled, phase 3 trial. , Lancet Neurol 21(12), 1099-1109.
- 13.Aldred J, Freire-Alvarez E, Amelin A V, Antonini A, Bergmans B et al.. Continuous Subcutaneous Foslevodopa/Foscarbidopa in Parkinson's Disease: Safety and Efficacy Results From a 12-Month, Single-Arm, Open-Label, Phase 3 Study. Neurol Ther 12(6), 1937-1958.
- 14.Katzenschlager R, Poewe W, Rascol O, Trenkwalder C, Deuschl G et al. (2021) Long-term safety and efficacy of apomorphine infusion in Parkinson's disease patients with persistent motor fluctuations: Results of the open-label phase of the TOLEDO study. Parkinsonism Relat Disord. 83, 79-85.
- 15. (2025) Agencia Española de Medicamentos y Productos Sanitarios. CIMA [Internet]. Ficha técnica (Summary of Product Characteristics) apomorfina 5 mg/ ml solución para perfusión.
- 16. (2025) Agencia Española de Medicamentos y Productos Sanitarios. CIMA [Internet]. Ficha Técnica (Summary of Product Characteristics) foslevodopa 240 mg/ml y foscarbidopa 12 mg/ml, solución para perfusión.
- 17. (2025) Consejo General de Colegios de Farmacéuticos de España [Internet]. Catálogo de Especialidades Farmacéuticas BOT Plus.
- 18.Henriksen T, Katzenschlager R, Bhidayasiri R, Staines H, Lockhart D et al.Practical use of apomorphine infusion in Parkinson's disease: lessons from the TOLEDO study and clinical experience. , J Neural Transm 130(11), 1475-1484.
- 19.Kempster P A, Frankel J P, Stern G M, Lees A J.Comparison of motor response to apomorphine and levodopa in Parkinson’s disease. , J Neurol Neurosurg Psychiatry 53(11), 1004-7.
- 20.NICE. (2025) Institute of Health Care and Excellence). Foslevodopa–foscarbidopa for treating advanced Parkinson’s with motor symptoms [Internet];.
- 21.HAS. (2025) Autorité de Santé): SCYOVA (foslevodopa/foscarbidopa) – Maladie de Parkinson [Internet];.
- 22.García-Fernández C, Vargas-Mendoza A K, López-López B, Blázquez-Estrada M, Suárez-San Martín ME.Nocturnal continuous subcutaneous infusion of apomorphine in advanced Parkinson's disease: a series of 37 cases. , Neurol 79(8), 217-221.
- 23.Dafsari H S, Martinez-Martin P, Rizos A, Trost M, MG Dos Santos Ghilardi et al.EuroInf 2: Subthalamic stimulation, apomorphine, and levodopa infusion in Parkinson's disease. , Mov Disord 34(3), 353-365.
- 24.Seeman P.Parkinson's disease treatment may cause impulse-control disorder via dopamine D3 receptors. , Synapse 69(4), 183-9.
- 25.Barbosa P, Lees A J, Magee C, Djamshidian A, Warner T T.A Retrospective Evaluation of the Frequency of Impulsive Compulsive Behaviors in Parkinson's Disease Patients Treated with Continuous Waking Day Apomorphine Pumps. Mov Disord Clin Pract. 4(3), 323-328.
- 26.Gomez-Inhiesto E, Acaiturri-Ayesta M T, Ustarroz-Aguirre I, Camahuali D, Urtaran-Laresgoiti M et al. (2020) Direct Cost of Parkinson's Disease: A Real-World Data Study of Second-Line Therapies. Parkinsons Dis. 9106026.
- 27.Carbone F, Djamshidian A, Seppi K, Poewe W. (2019) Apomorphine for Parkinson's Disease: Efficacy and Safety of Current and New Formulations. CNS Drugs. 33(9), 905-918.