
Disseminated Mucormycosis Diagnosed by Urine Microscopy in a Patient with Relapsed Acute Lymphoblastic Leukemia: A Case Report
Abstract
Background
Mucormycosis is a rapidly progressive invasive fungal infection associated with high mortality in patients with hematological malignancies such as Acute Lymphoblastic Leukemia(ALL). Early diagnosis is challenging because clinical and radiological findings are often nonspecific, and tissue biopsy may be difficult in immunocompromised patients. Microbiological identification using rapid, low-cost techniques can therefore play a critical role in early detection.
Case Presentation
We report a 28-year-old male with relapsed pre-B acute lymphoblastic leukemia receiving salvage chemotherapy who developed disseminated mucormycosis with pulmonary and renal involvement. Routine urine potassium hydroxide (KOH) microscopy unexpectedly demonstrated broad, ribbon-like, aseptate fungal hyphae suggestive of Mucorales. This rare finding was reconfirmed on repeat urine examination. Urine fungal culture yielded growth of Mucor species, and lactophenol cotton blue (LPCB) staining confirmed characteristic morphology. Subsequent imaging revealed bilateral emphysematous pyelonephritis and pulmonary cavitary and nodular lesions. The diagnosis was further supported by isolation of Mucor species from renal pus and lung biopsy specimens.
Management and Outcome
Based on early microbiological evidence, antifungal therapy was initiated promptly according to European Conference on Infections in Leukemia (ECIL) guidelines. The patient received high-dose liposomal amphotericin B, followed by the addition of isavuconazole. Surgical intervention was not feasible due to extensive bilateral pulmonary and renal involvement. With early, guideline-directed antifungal therapy and supportive care, the patient demonstrated clinical improvement, stabilization of renal function, and rising serum albumin levels.
Conclusion
This case highlights the pivotal role of urine KOH microscopy and fungal culture in the early diagnosis of disseminated mucormycosis. Rapid microbiological identification enabled timely initiation of appropriate antifungal therapy, contributing to clinical stabilization in a high-risk patient with relapsed ALL. Simple, accessible microbiological techniques should be considered valuable diagnostic tools in suspected invasive fungal infections when tissue diagnosis is delayed or not feasible.
Article Information
- Received
- Accepted
- Published
Academic Editor: N. R. Rajagopalan, Assistant Professor, Department of Chemistry, St. Joseph’s College of Engineering, Chennai
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2026 Bhavini Shah, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Nidhi Rao, Clinical Pharmacologist —
Competing Interests
The authors have no conflict of interest to declare.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Citation:
Introduction
Acute lymphoblastic leukemia (ALL) is an aggressive hematological malignancy that predominantly affects children and young adults and is associated with favorable outcomes when treated with contemporary risk-adapted chemotherapy protocols 1, 2. However, relapsed ALL continues to pose a major therapeutic challenge, often requiring intensive salvage chemotherapy and prolonged corticosteroid exposure, leading to profound immunosuppression and increased susceptibility to opportunistic infections 2, 3.
Invasive fungal infections are a significant cause of morbidity and mortality in patients with ALL, particularly in the relapsed or refractory setting 4. Among these, mucormycosis is a rare but rapidly progressive angioinvasive fungal infection caused by fungi of the order Mucorales5. It primarily affects immunocompromised hosts, including patients with hematological malignancies, and is associated with high mortality rates despite advances in antifungal therapy 6. Pulmonary and rhino-orbito-cerebral forms are most frequently reported; however, disseminated disease with renal involvement is uncommon and often underdiagnosed 6, 7.
Early diagnosis of mucormycosis is challenging due to nonspecific clinical manifestations and limited sensitivity of routine diagnostic modalities 5, 7. While histopathological confirmation remains the gold standard, rapid and accessible techniques such as direct microscopy and fungal culture from clinical specimens can play a crucial role in early detection, particularly in disseminated disease where tissue sampling may be difficult 7, 8.
Here, we report a case of disseminated mucormycosis involving the lungs and kidneys in a patient with relapsed pre-B acute lymphoblastic leukemia, diagnosed through urine KOH microscopy and urine fungal culture, and successfully managed with ECIL-guided antifungal therapy 8, 9, 10. This case highlights the importance of early suspicion, detailed clinical history by patient and reletives, and timely guideline-directed treatment in improving outcomes in high-risk ALL patients.
Case presentation
A 28-year-old male was diagnosed with relapsed Pre-B acute lymphoblastic leukemia at Rajkot. He received chemotherapy according to the BFM 2002 protocol and completed treatment in October 2023, and maintenance was completed after 2 and half years. Subsequently, the patient developed disease relapse. Flow cytometric analysis confirmed pre-B ALL. Cytogenetic evaluation demonstrated a normal karyotype (46, XY). Next-generation sequencing (NGS) revealed a MEF2D-BCL9 fusion along with multiple copy number variations involving chromosomes 10, 12, and 19, indicating high-risk disease biology.
In view of relapsed disease, he was started on salvage therapy using bortezomib-based Children’s Oncology Group (COG) protocol, with a treatment plan to proceed to allogeneic stem cell transplantation or CAR-T cell therapy based on response. The patient received prednisolone 40 mg/day, vincristine (1.4mg/m2 on Days 1, 8, and 15), Bortezomib (1.3 mg/m² on Days 1, 8, and 15), Doxorubicin (60 mg/m² on Day 1), Peg-asparaginase (1000 units/m² on Days 3, 10, and 18) (Figure 1).
Figure 1. Flow cytometric result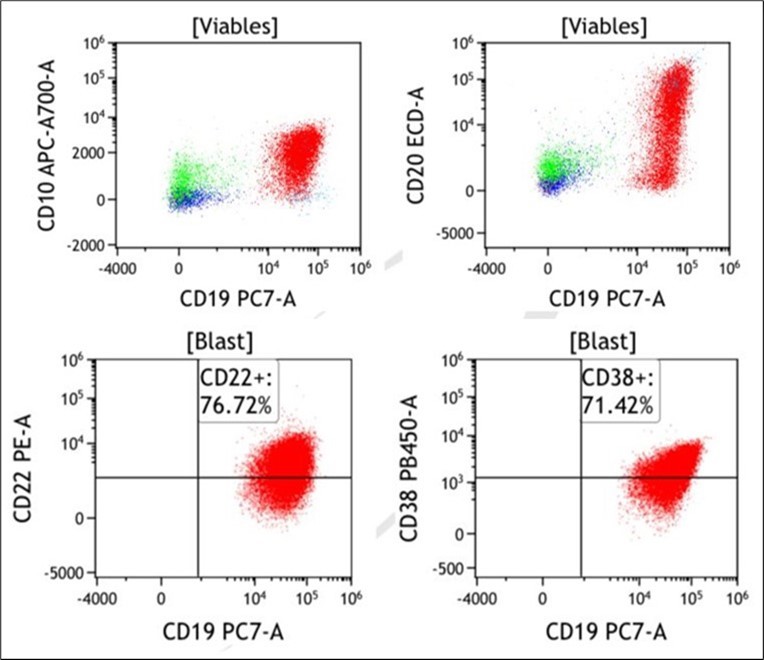
Download figure
His clinical course was relatively uneventful for the first three weeks of therapy. After three weeks, he developed acute liver injury, which was attributed to the ongoing chemotherapy. With supportive care, his bilirubin levels and transaminases began to resolve. He subsequently developed minimal cough and fever, which were initially attributed to a viral illness, along with the presence of white patches in the oral cavity. In response, steroid tapering was initiated, and oral posaconazole was started empirically. Over the next week, the patient developed urinary urgency, lower abdominal pain, and fever (101°F) and presented to the hospital for further treatment. During hospitalization, urine potassium hydroxide (KOH) examination demonstrated the presence of broad, aseptate fungal hyphae suggestive of Mucor species.
Following this finding, a detailed retrospective history was obtained from the patient and his relatives. It was then revealed that approximately 10 days after the initiation of steroid tapering, the patient experienced right-sided chest pain, cough, and one to two episodes of haemoptysis, which had not been reported earlier. Subsequently, the patient developed hypoalbuminemia and acute kidney injury (AKI).
Microbiology
KOH preparation
A Urine KOH test identified the presence of septate Broad, ribbon-like, aseptate fungal hyphae suggestive of mucormycosis. A repeat urine sample was also requested on the next day to reconfirm this rare, unexpected finding. KOH for the scond sample also showed septate Broad, ribbon-like, aseptate fungal hyphae suggestive of mucormycosis. Urine Fungal culture shows Growth of Mucor species and Candida albicans. In the view of this microbiological finding, Imaging was requested.
Figure 2. Microbiological findings suggestive of mucormycosis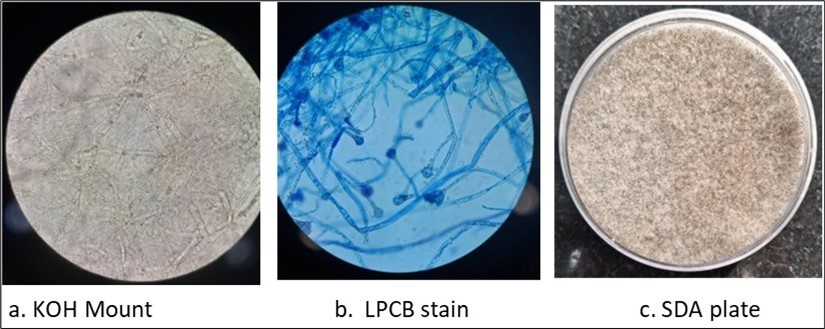
Download figure
Potassium Hydroxide (KOH) Mount – Tissue Sample (Figure 2.a)
A small fragment of the tissue specimen was placed on a clean glass slide. The tissue was not minced or homogenized prior to processing to avoid disruption of the fragile hyphae of Mucorales. One to two drops of 10–20% potassium hydroxide (KOH) were added, and a coverslip was gently placed. The preparation was allowed to stand at room temperature for 5 to 7 minutes to facilitate digestion and clearing of tissue elements. 12, 14
The slide was examined under low (10×) and high (40×) power magnification using a light microscope. 12, 14 The preparation demonstrated broad, aseptate to pauciseptate hyphae with right-angled branching, consistent with mucormycosis.12, 14
Culture procedure (Figure 2.c)
Fresh tissue obtained from the affected site was received in a sterile container and processed immediately. The tissue was not minced or homogenized prior to culture to prevent damage to the fragile hyphae of Mucorales. Instead, small tissue fragments were directly inoculated onto Sabouraud dextrose agar (SDA) and incubated at 25°C and 37°C. The cultures were examined daily. Rapidly growing, fluffy, cottony white to gray colonies were observed, Suggestive of Mucorales infection. 12, 13
lactophenol cotton blue (LPCB) stain (Figure 2.b)
For further identification, a tease mount from the fungal colony grown on SDA was prepared using lactophenol cotton blue (LPCB) stain. Microscopic examination revealed broad, ribbon-like aseptate hyphae with sporangiophores and sporangia, confirming the isolate as a member of the order Mucorales.12, 13 Based on direct microscopy, culture characteristics, and LPCB morphology, the fungal isolate was identified as Mucor species, in accordance with standard mycological diagnostic criteria. 12, 16
Radiology
Imaging revealed bilateral emphysematous pyelonephritis, a cavitary lesion in the right mid-zone of the lung, an ipsilateral pleural effusion, and bilateral lung nodularities. A DJ stent was placed to drain the pus from the kidney, pleural fluid tapping was performed, and a biopsy was taken from the lung's cavitary lesion. The pus from the kidney and the lung biopsy both confirmed the presence of Mucor, although the pleural fluid did not show other infections.
Management
The patient was initiated on intravenous liposomal amphotericin B for suspected invasive fungal infection in the setting of acute lymphoblastic leukemia. Liposomal amphotericin B (Amphomul) was initially administered at a dose of 300 mg once daily intravenously, which was subsequently escalated to 350 mg once daily based on clinical response and tolerability. Supportive management included intravenous albumin infusion at a rate of 20 mL/hour, administered once daily to address hypoalbuminemia, and intravenous vitamin K (10 mg once daily) for correction of coagulopathy.
The patient was closely monitored throughout hospitalization for renal function, electrolyte disturbances, and treatment-related adverse effects.
Due to the bilateral involvement of both the lungs and kidneys, surgical intervention was not considered feasible by the relative. The patient was started on a combination of Liposomal Amphotericin B and Isavuconazole. After two weeks of this treatment, the patient is doing reasonably well, and his creatinine levels are beginning to decrease and Albumin level is rising.
Discussion
Patients with acute lymphoblastic leukemia (ALL), particularly those with relapsed disease, are at high risk for invasive fungal infections due to profound immunosuppression caused by intensive chemotherapy, prolonged neutropenia, and corticosteroid exposure. Among these infections, mucormycosis is uncommon but highly aggressive, with mortality rates exceeding 40–50% in patients with hematological malignancies 4, 6.
Relapsed ALL further amplifies this risk because of cumulative treatment-related toxicity, immune dysfunction, and metabolic derangements. Mucormycosis in ALL most frequently involves the lungs or rhino-orbito-cerebral region; however, disseminated disease with renal involvement, as seen in this patient, is rare and reflects severe immune compromise 6, 7. The angioinvasive nature of Mucorales leads to vascular thrombosis, tissue necrosis, and rapid progression, making early recognition critical for survival 5.
Early diagnosis of mucormycosis remains challenging, as clinical and radiological findings are often nonspecific, and tissue biopsy is frequently difficult in patients with thrombocytopenia or critical illness. While histopathology remains the diagnostic gold standard, direct microscopy and fungal culture from clinical specimens play an important supportive role, particularly in disseminated disease 7, 8.
In this case, identification of broad, ribbon-like, aseptate hyphae on urine KOH examination, along with growth of Mucor species on urine fungal culture, was instrumental in early diagnosis. Detection of Mucor in urine is uncommon but strongly suggestive of renal or disseminated mucormycosis, especially when correlated with imaging findings such as emphysematous pyelonephritis. These rapid, low-cost diagnostic modalities enabled early initiation of targeted antifungal therapy prior to tissue confirmation, emphasizing their value in high-risk ALL patients 7, 8.
The key learning point in this case was the absence of an initially reported history of respiratory illness. It was only after the microbiology laboratory reported features suggestive of mucormycosis on KOH examination of the urine sample that a detailed re-enquiry was made. At that time, the patient’s relative disclosed a history of respiratory symptoms for the preceding 15 days, which had not been volunteered earlier. This crucial information subsequently prompted targeted radiological evaluation of the lungs and kidneys, leading to further diagnostic clarification.
Management of mucormycosis in patients with ALL requires urgent initiation of antifungal therapy, correction of underlying predisposing factors, and surgical intervention when feasible. According to ECIL (European Conference on Infections in Leukemia) guidelines, high-dose liposomal amphotericin B is the first-line treatment for mucormycosis and carries a strong recommendation (A-II) for patients with hematological malignancies 9.
ECIL further recommends early initiation of antifungal therapy without delay for definitive histopathological confirmation in patients with strong clinical suspicion, as treatment delay is associated with significantly increased mortality. Isavuconazole and posaconazole are recommended as salvage or step-down therapy (B-II), particularly in patients with renal impairment or intolerance to amphotericin B 9, 10.
In the present case, surgical intervention was not feasible due to extensive bilateral pulmonary and renal involvement. Therefore, management followed ECIL-guided medical therapy using liposomal amphotericin B, followed by addition of isavuconazole, which is supported by ECIL recommendations for severe or disseminated mucormycosis when surgical options are limited. Isavuconazole offers the advantage of a favorable safety profile, predictable pharmacokinetics, and reduced nephrotoxicity, making it particularly suitable in ALL patients with evolving renal dysfunction 9, 10, 11.
The patient’s clinical improvement, stabilization of renal function, and rising serum albumin levels highlight the importance of early ECIL-guided antifungal therapy and individualized treatment strategies in managing mucormycosis complicating ALL.
Conclusion
Patients with relapsed acute lymphoblastic leukemia are at a high risk of developing invasive fungal infections, including mucormycosis, due to profound immunosuppression related to intensive chemotherapy and corticosteroid exposure. This case highlights disseminated mucormycosis with pulmonary and renal involvement as a rare but life-threatening complication in an ALL patient. Early identification of Mucorales through urine KOH microscopy and urine fungal culture proved crucial in establishing the diagnosis and enabling prompt initiation of antifungal therapy. Management in accordance with ECIL recommendations, including early administration of high-dose liposomal amphotericin B and adjunctive isavuconazole when surgical intervention was not feasible, resulted in clinical stabilization and organ function improvement. This case underscores the importance of maintaining a high index of suspicion for mucormycosis in high-risk ALL patients and demonstrates that early, guideline-directed antifungal therapy can be lifesaving even in disseminated disease.
References
- 1.Pui C H, Mullighan C G, Evans W E, Relling M V. (2012) Pediatric acute lymphoblastic leukemia: where are we going and how do we get there?. , Blood 120(6), 1165-1174.
- 2.Fielding A K. (2011) Treatment of adults with acute lymphoblastic leukemia. Hematology Am Soc Hematol Educ Program. 381-389.
- 3.Loh M L, Zhang J, Harvey R C. (2013) Tyrosine kinome sequencing of pediatric acute lymphoblastic leukemia. , Blood 121(3), 485-488.
- 4.Pagano L, Caira M, Candoni A. (2010) Invasive aspergillosis and mucormycosis in patients with acute leukemia. , Haematologica 95(4), 644-650.
- 5.Spellberg B, Edwards J Jr, Ibrahim A. (2005) Novel perspectives on mucormycosis. Clin Microbiol Rev. 18(3), 556-569.
- 6.Roden M M, Zaoutis T E, Buchanan W L. (2005) Epidemiology and outcome of zygomycosis. Clin Infect Dis. 41(5), 634-653.
- 7.Petrikkos G, Skiada A, Lortholary O. (2012) Epidemiology and clinical manifestations of mucormycosis. Clin Infect Dis. 54(Suppl 1):S23–S34.
- 8.Skiada A, Pavleas I, Drogari-Apiranthitou M. (2020) Epidemiology and diagnosis of mucormycosis. , J Fungi (Basel) 6(4), 265.
- 9.Cornely O A, Arikan-Akdagli S, Dannaoui E. (2014) ESCMID and ECIL guidelines for the diagnosis and management of mucormycosis. Clin Microbiol Infect. 20, 5-26.
- 10.Cornely O A, Alastruey-Izquierdo A, Arenz D. (2019) Global guideline for the diagnosis and management of mucormycosis. Lancet Infect Dis.
- 11.Marty F M, Ostrosky-Zeichner L, Cornely O A. (2016) Isavuconazole treatment for mucormycosis. Lancet Infect Dis. 16(7), 828-837.
- 13.Larone D H. (2018) Medically Important Fungi: A Guide to Identification. 6th ed. , Washington, DC:
- 14.Walsh T J, Gamaletsou M N, McGinnis M R, Hayden R T, Kontoyiannis D P. (2012) Early clinical and laboratory diagnosis of invasive mucormycosis. Clin Infect Dis. 54(Suppl 1):S55–S60.